Commonwealth Fund: The U.S. Healthcare System Is an International Embarrassment
What is wrong with the US healthcare system and what we have done to fix it
Introduction
We are going to examine what the Commonwealth Fund thinks is wrong with the US healthcare system, point by point and detail a solution for each in a ‘Problem’ and ‘Solution’ format.
The Commonwealth Fund
The Commonwealth Fund is a private U.S. foundation that aims to “promote a high-performing health care system with better access, improved quality, and greater efficiency, particularly for vulnerable populations such as low-income people, the uninsured, and people of color.”
The Article
In January of 2023, the Commonwealth Fund published U.S. Health Care from a Global Perspective, 2022: Accelerating Spending, Worsening Outcomes. This article deals mostly with mortality as it relates to healthcare spending; it is not really about medicine, and we here at Sentia Health are kind of in the same business. Doctors know what to do, it is the bankers running health insurance that are killing people.
The Commonwealth Fund’s Highlights of the Problem
In the previous edition of U.S. Health Care from a Global Perspective, they reported that people in the United States experience the worst health outcomes overall of any high-income nation. Americans are more likely to die younger, and from avoidable causes, than residents of peer countries.
Between January 2020 and December 2021, life expectancy dropped in the U.S. and other countries. With the pandemic a continuing threat to global health and well-being, we have updated our 2019 cross-national comparison of health care systems to assess U.S. health spending, outcomes, status, and service use relative to Australia, Canada, France, Germany, Japan, the Netherlands, New Zealand, Norway, South Korea, Sweden, Switzerland, and the United Kingdom. We also compare U.S. health system performance to the OECD average for the 38 high-income countries for which data are available. The data for our analysis come from the Organization for Economic Co-operation and Development (OECD) and other international sources (see “How We Conducted This Study” for details).
For every metric we examine, we used the latest data available. This means that results for certain countries may reflect the height of the COVID-19 pandemic, when mental health conditions were surging, essential health services were disrupted, and patients may not have received the same level of care.
Highlights
- Health care spending, both per person and as a share of GDP, continues to be far higher in the United States than in other high-income countries. Yet the U.S. is the only country that doesn’t have universal health coverage.
- The U.S. has the lowest life expectancy at birth, the highest death rates for avoidable or treatable conditions, the highest maternal and infant mortality, and among the highest suicide rates.
- The U.S. has the highest rate of people with multiple chronic conditions and an obesity rate nearly twice the OECD average.
- Americans see physicians less often than people in most other countries and have among the lowest rate of practicing physicians and hospital beds per 1,000 population.
- Screening rates for breast and colorectal cancer and vaccination for flu in the U.S. are among the highest, but COVID-19 vaccination trails many nations.
Our Conclusions about the Highlights
It seems to us at Sentia that these problems all boil down to two root cause categories:
- Money
- Education
If we bring down the cost of health insurance (notice that is not the care itself, that is a different subject that we will discuss in a future episode) and educate the patient on behavior that causes and exacerbates chronic disease then we would be at par or better than criminally expensive universal health coverage that we know from experience in the UK and Canada isn’t a viable option.
Findings
Below are the findings of the Commonwealth article with our comments in the conclusions section following.
Health Care Spending and Coverage

Figure 1 - World Healthcare Spending
In all countries, health spending as a share of the overall economy has been steadily increasing since the 1980s, as spending growth has outpaced economic growth. This growth is in part because of medical technologies, rising prices in the health sector, and higher demand for services. In 2020, when the COVID-19 pandemic began, health care spending rose rapidly in nearly all countries, as governments sought to mitigate the spread of the disease through COVID testing, vaccine development, relief funds, and other measures. Since then, spending has slowed but still remains higher from years prior.
In 2021, the U.S. spent 17.8 percent of gross domestic product (GDP) on health care, nearly twice as much as the average OECD country.

Figure 2 - US Spends 3-4 times more on healthcare than South Korea, New Zealand and Japan
Health spending per person in the U.S. was nearly two times higher than in the closest country, Germany, and four times higher than in South Korea. In the U.S., that includes spending for people in public programs like Medicaid, the Children’s Health Insurance Program, Medicare, and military plans; spending by those with private employer-sponsored coverage or other private insurance; and out-of-pocket health spending.
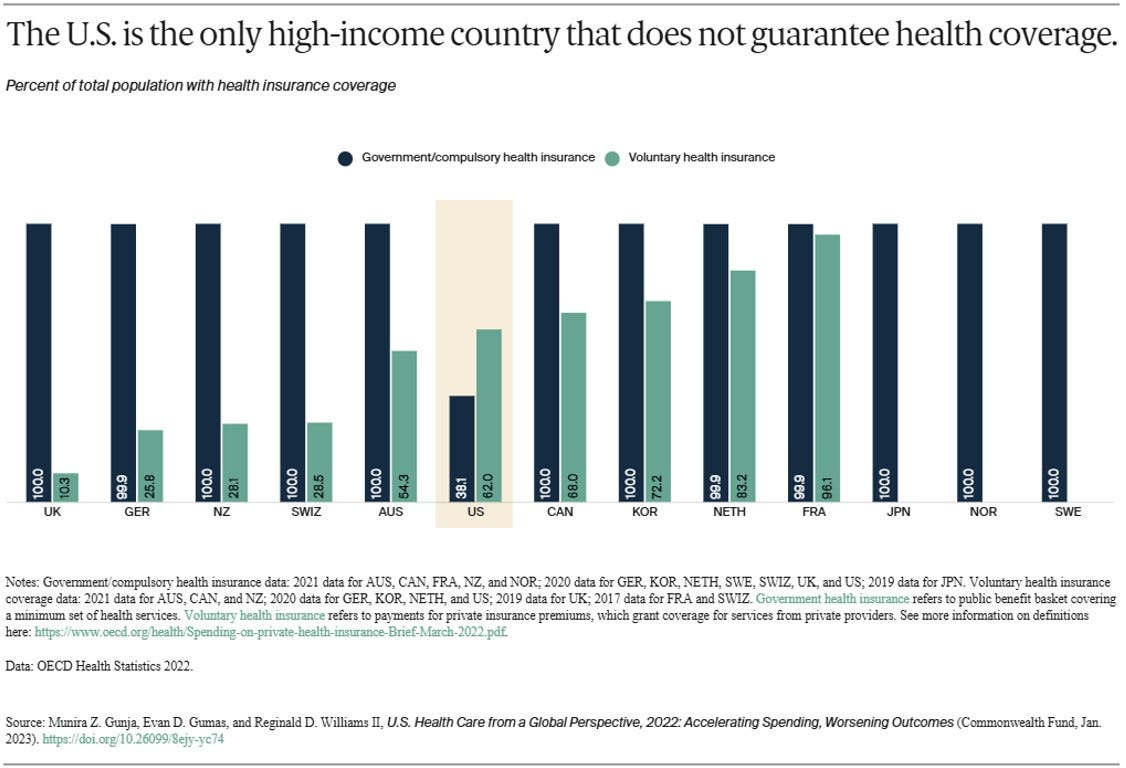
Figure 3 - The US is the only country that doesn’t guarantee health coverage
All countries in this analysis, except the U.S., guarantee government, or public, health coverage to all their residents. In addition to public coverage, people in several of the countries have the option to also purchase private coverage. In France, nearly the entire population has both private and public insurance.
In 2021, 8.6 percent of the U.S. population was uninsured. The U.S. is the only high-income country where a substantial portion of the population lacks any form of health insurance.
Our Conclusion on World Healthcare Spending
These charts are all misleading. The text below them is simply wrong. The U.S. simply has more money to spend on heath care and therefore this is going to skew us toward the high end. This, therefore isn’t as bad as it looks. It is bad, though, and of course could of course be better. Let's take a look at how.
Let’s consider that in the US about half your health coverage dollar, 47%, is wasted by big insurance. Add to that the fact that EMR, medical coding and compliance reporting combined, cost the average practitioner $77,000 each. If we had a new breed of insurance company that provides the EMR, thusly eliminating medical coding, and automating compliance reporting, then we can conclude that we would save at least half from the cost of health coverage. The stated 17.8% of GDP then, would become something on the order of 8.9%, on par with the least cost systems in South Korea at 8.8% of GDP.
This is what we at Sentia are working on. We can replace everything the big insurance companies do, with automation, and simply charge a Netflix or Amazon like subscription fee of $10 per month (plus the actual incurred risk) to manage the data and pay for your healthcare. These are real numbers. The difference between what the rest of the world is doing and what we are doing is automation.
Health Outcomes

Despite high U.S. spending, Americans experience worse health outcomes than their peers around world. For example, life expectancy at birth in the U.S. was 77 years in 2020 — three years lower than the OECD average. Provisional data shows life expectancy in the U.S. dropped even further in 2021.
In the U.S., life expectancy masks racial and ethnic disparities. Average life expectancy in 2019 for non-Hispanic Black Americans (74.8 years) and non-Hispanic American Indians or Alaska Natives (71.8 years) is four and seven years lower, respectively, than it is for non-Hispanic whites (78.8 years).
Meanwhile, life expectancy for Hispanic Americans (81.9 years) is higher than it is for whites and similar to life expectancy in the Netherlands, New Zealand, and Canada. As a group, Asian Americans have a higher life expectancy (85.6 years) than people in Japan.

Figure 5 - US Avoidable Deaths are higher than OECD average
Avoidable mortality refers to deaths that are preventable and treatable. Preventable deaths can be avoided through effective public health measures and through primary prevention, such as nutritional diet and exercise. Treatable mortality can be avoided mainly through timely and effective health care interventions, including regular exams, screenings, and treatment. Since 2015, avoidable deaths have been on the rise in the U.S., which had the highest rate in 2020 of all the countries in our analysis.
Figure 6 - US has the highest rate of infant mortality
In 2020, the infant mortality rate in the U.S. was 5.4 deaths per 1,000 live births, the highest rate of all the countries in our analysis. In contrast, there were 1.6 deaths per 1,000 live births in Norway.
Women in the U.S. have long had the highest rate of maternal mortality related to complications of pregnancy and childbirth. In 2020, there were nearly 24 maternal deaths for every 100,000 live births in the U.S., more than three times the rate in most of the other high-income countries we studied. A high rate of cesarean section, inadequate prenatal care, and socioeconomic inequalities contributing to chronic illnesses like obesity, diabetes, and heart disease may all help explain high U.S. infant and maternal mortality.
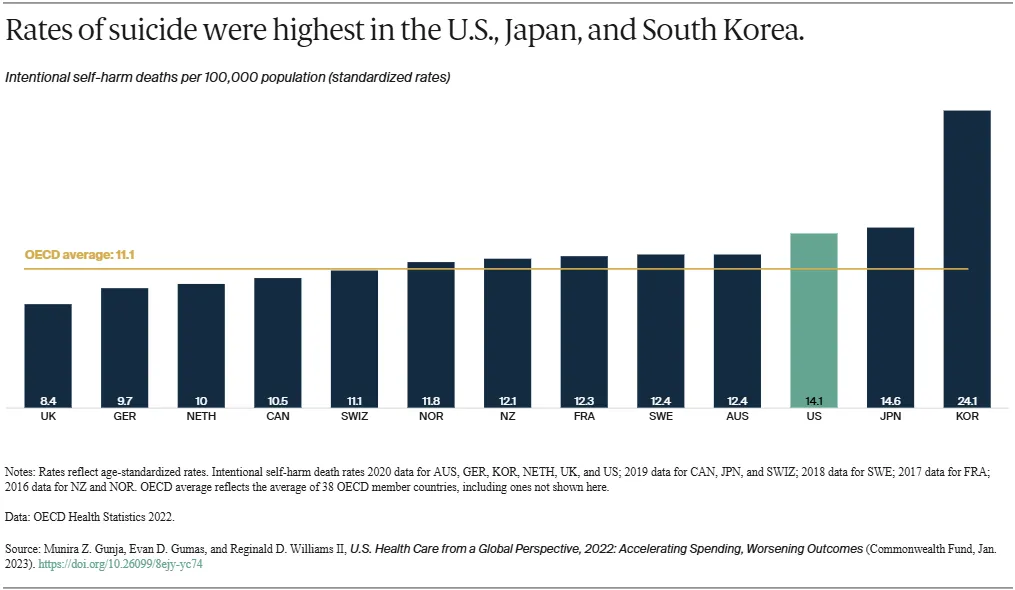
Figure 7 - Rates of suicide were highest in US, Japan and South Korea
Elevated suicide rates, which have dramatically increased during the COVID-19 pandemic, can indicate a high burden of mental illness. The U.S. has the third-highest suicide rate, while the U.K. has the lowest — nearly half the U.S. rate.

Figure 8 - Deaths from assault are highest in the US
The U.S. is an outlier in deaths from physical assault, which includes gun violence. Its 7.4 deaths per 100,000 people is far above the OECD average of 2.7, and at least seven times higher than all other high-income countries in our study, except New Zealand.
Our Conclusion about Health Outcomes
These illustrations are a little disingenuous, however, they could be mostly compensated for with less expensive health coverage and some patient education. If our new health insurance company also provided health and wellness functionality, and it does, with the teeth to say “if you behave this way you will not receive the discounts that people who DON’T behave this way do,” then we incentivize a healthier lifestyle and can check up on progress via measurements, lab data and blood work. Let’s think about smoking or a sedentary lifestyle. These are easily measurable and we can provide the carrot, in the form of an insurance discount, that incentivizes healthy living. If we test and find nicotine in the bloodstream the discount is removed. If we check the patient’s resting heart rate and HDL we have a good indication of his or her progress toward a healthy lifestyle. Everything else in this section can be attributed to mental health. Life expectancy and avoidable deaths are both due to a less-than-fully educated population and is easily mitigated with the health and wellness package discussed above. Here is a sample of our patient education:

Figure 9 - Sample Generated Patient Education
The mental health part of this is a little trickier and we have to assume that is due to culture. Other places don’t have this macho, “don’t know don’t care, I’ll do what I like” attitude that we do here. We are working on a new module that will ask mental health questions and assign reading and homework based on the answers. Since this is part and parcel of the application, we can tell who has taken the tests and done the homework, and incentivize that in the same way we do the health and wellness. Of course this isn’t a substitute for therapy, but with this we can identify the people in need of more involved help and get them access to a mental health professional.
This proves that our assertion that money, or affordability of coverage, and education are they key factors in determining positive medical outcomes.
In a completely unrelated note, we find it is interesting that the two lowest spending countries have the highest rates of suicide. If they had an automated mental health package like we described, maybe this wouldn’t be the case.
Health Status

Obesity is a key risk factor for chronic conditions such as diabetes, hypertension and other cardiovascular diseases, and cancer. Issues that contribute to obesity include unhealthy living environments, less-regulated food and agricultural sectors, lower socioeconomic status, and higher rates of behavioral health problems.
The U.S. has the highest obesity rate among the countries we studied, where data was available — nearly two times higher than the OECD average.

In 2020, three of 10 U.S. adults surveyed said at some point in their lifetime they had been diagnosed with two or more chronic conditions such as asthma, cancer, depression, diabetes, heart disease, or hypertension. No more than a quarter of residents in the other countries studied reported the same, and the U.S. rate was nearly twice as high as France’s.

Since the start of the COVID-19 pandemic, more people in the U.S. have died from the coronavirus than any in any other high-income country. For every 1 million cases between January 22, 2020, and January 18, 2023, there were more than 3,000 deaths in the U.S.
Our Conclusion to the Health Status
The graphics presented are interested in obesity, multiple chronic conditions, and COVID-19 Death rates. All of these things can be mitigated by proper patient education and the carrot-and-stick approach. If one health insurance company is charging you less than half what the others are you will use them. If that company offers significant discounts for science based, lab tested, healthy living, patients will get healthier. If they don’t, they will pay for their lack of understanding and that payment will cause the cost to go down for the rest of us.
This is not difficult. If you want people to do something you incentivize it. You give them a reason to do what it is that you want them to do. Then you explain, step by step and in detail exactly what you need them to do and they will go do it.
We here at Sentia are unclear how we combat the un-belief in science and the refusal to take the vaccine for COVID-19. Probably though, with the resources a major insurer possesses, and advertising campaign stating the truth about science and the vaccination would have some impact, particularly on social media or direct electronic communication like email or SMS (text) messages. As a payer, we would actually be incurring expense for an efficacious vaccination that will keep the patient healthy, reduce risks and reduce costs for everyone. If the vaccine didn’t work or had some nefarious purpose, we wouldn’t be for it, as we have to pay for it.
Healthcare Use
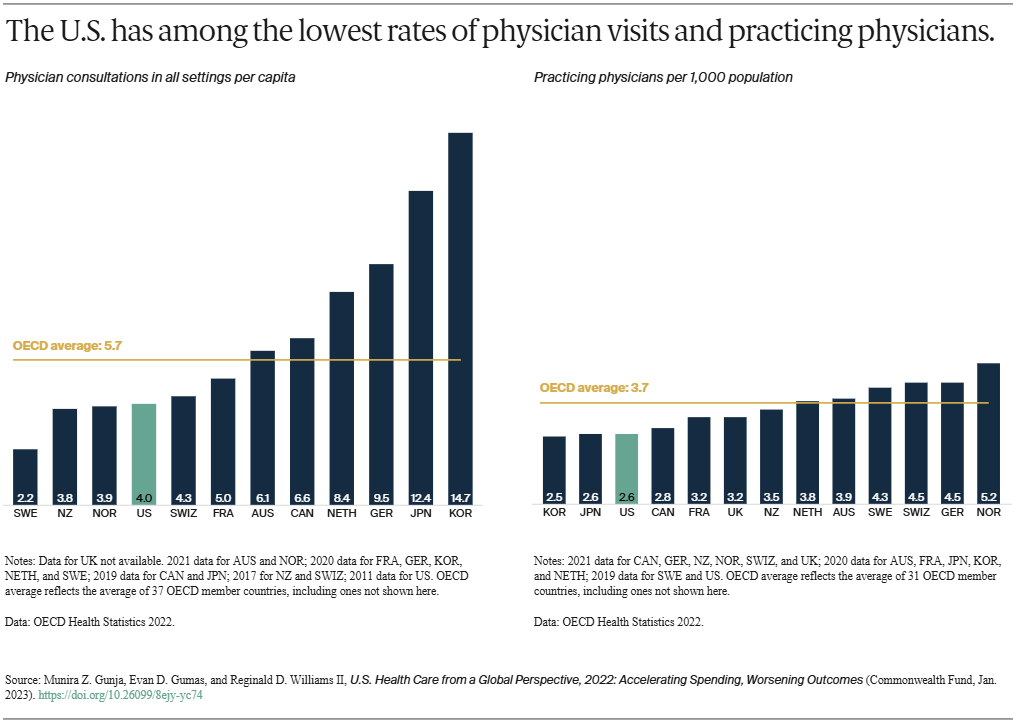
While U.S. health care spending is the highest in the world, Americans overall visit physicians less frequently than residents of most other high-income countries. At four visits per person per year, Americans see the doctor less often than the OECD average.
Less-frequent physician visits may be related to the comparatively low supply of physicians in the U.S., which is below the average number of practicing physicians in OECD countries.
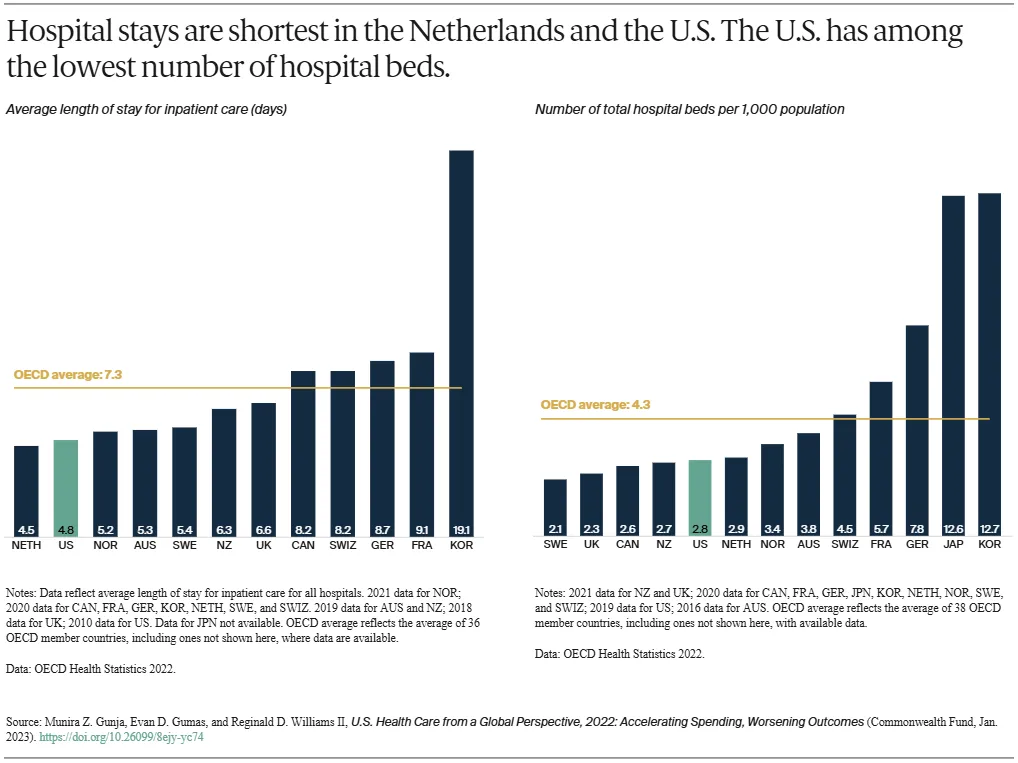
The average length of a hospital stay in the U.S. for all inpatient care was 4.8 days, far lower than the OECD average. The U.S. had 2.8 hospital beds per 1,000 population, lower than the OECD average of 4.3.

More than two-thirds of older Americans receive the flu vaccine, similar to older residents of several other high-income countries, and more than the OECD average.
The U.S., however, has one of the lowest COVID-19 vaccination rates among high-income countries. As of January 2023, 69 percent of the population were fully vaccinated, compared to 86 percent in South Korea, although rates are regularly being updated.

The U.S. does relatively well with cancer prevention. This is likely a reflection of extensive screening and detection, a key to diagnosing breast and colorectal cancers early and beginning treatment in a timely manner.
The U.S. and Sweden had the highest number of breast cancer screenings among women ages 50 to 69, notably higher than the OECD average. In contrast, just 43 percent of women ages 50 to 69 were screened in France. When it comes to colorectal cancer screening, the U.S. exceeded the OECD average and had among the highest rates.
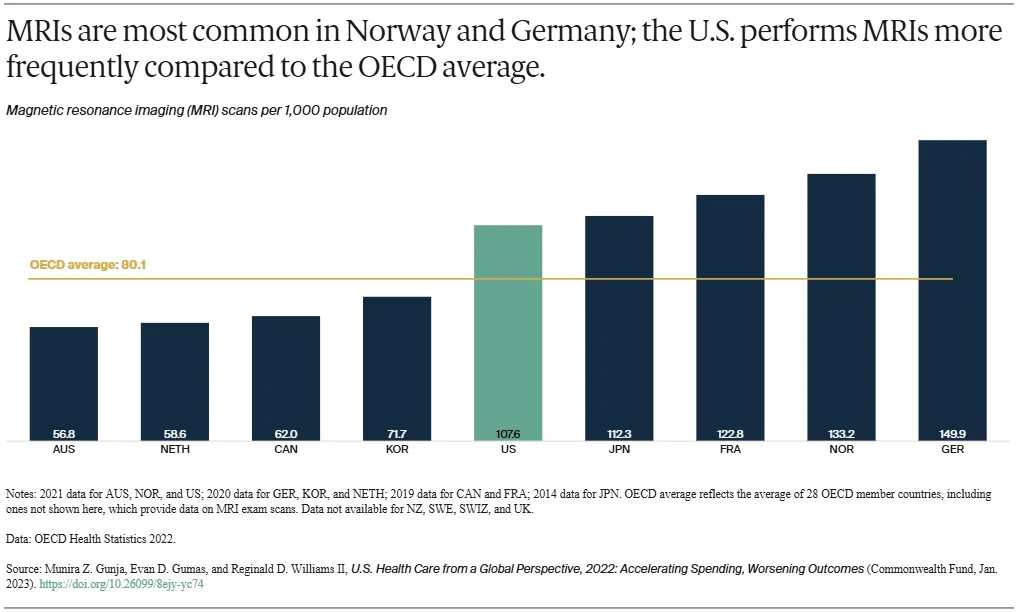
Magnetic resonance imaging, or MRI, is a common and effective imaging technique for diagnosing and tracking the treatment of a variety of illnesses. The countries that use these specialized scans the most are the U.S., Japan, France, Norway, and Germany, with more than 100 scans per 1,000 people.
The U.S. has a high number of MRI units available to physicians, about 38 units for every 1 million people in 2018. That’s the second-highest rate in the world behind Japan, which has 51.7 units per 1 million people.
While their clinical benefit as a diagnostic tool is well documented, MRIs are particularly expensive in the U.S., averaging $1,119. That’s 42 percent more than the U.K.’s average cost and 420 percent more than Australia’s. And while MRIs are accessible in the U.S., Americans spend far more on them than their international peers do.

Globally, rates of hip replacement are increasing as populations age and develop conditions like osteoarthritis — the leading reason for the procedure, which can substantially improve an individual’s quality of life. Hip replacements are an important indicator of the prevalence of osteoarthritis in a population.
Our Conclusion to Health Care Use
Clearly, when insurance pays for care, the US patients take advantage of it. The physician visits are low, probably due to the impediments and hurdles placed by old, legacy insurance companies, like co-pays and co-insurance. If the patient has to shell out for a visit, they might just say “it’s probably nothing.” And wait to see if it clears up on its own.
Influenza vaccinations, breast and colorectal cancer screenings, MRIs, and hip replacement incidence in the US are all world leading helping us to draw the conclusion that people are willing to engage and change behavior, if their care is covered and they are informed of what exactly to do. Again, by lowering the cost and the impediments to seeing a doctor on a regular basis and by educating the patient on what they should be doing, can we rectify this situation.
This is precisely what we are doing at Sentia Health. With our $10 per month (plus the actual cost of the incurred risk) healthcare-as-a-subscription service, we can save the patient at least half of the cost of their coverage AND automatically prescribe education based on lab work and procedures performed. This is the only viable way to not only retain the best doctors in the world, but make care in the US both the best by utilizing those doctors in a financially efficient manner and educating the patients on their own personal responsibility in relation to their care.
With the other parts of our service, care becomes healthcare-as-a-platform that includes all that a patient, practitioner and practice or hospital needs. We will discuss exactly what those are in a moment.
Discussion
While the United States spends more on health care than any other high-income country, the nation often performs worse on measures of health and health care. For the U.S., a first step to improvement is ensuring that everyone has access to affordable care. Not only is the U.S. the only country we studied that does not have universal health coverage, but its health system can seem designed to discourage people from using services.
Affordability remains the top reason why some Americans do not sign up for health coverage, while high out-of-pocket costs lead nearly half of working-age adults to skip or delay getting needed care. The Inflation Reduction Act, which will help reduce the high cost of certain drugs and cap out-of-pocket costs for older Americans, is a step in the right direction. But it will take much more to make health care as easy to access as it is in other high-income countries.
A second step is containing costs. Other countries have achieved better health outcomes while spending much less on health care overall. In the U.S., high prices for health services continue to be the primary driver of this elevated spending. U.S. policymakers and health systems could look to some of the approaches taken by other nations to contain overall health spending, including health care and administrative costs.
A third step is better prevention and management of chronic conditions. Critical to this is developing the capacity to offer comprehensive, continuous, well-coordinated care. Decades of underinvestment, along with an inadequate supply of health care providers, have limited many Americans’ access to effective primary care.
The findings of our international comparison demonstrate the importance of a health care system that supports chronic disease prevention and management, the early diagnosis and treatment of medical problems, affordable access to health care coverage, and cost containment — among the key functions of a high-performing system. Other countries have found ways to do these things well; the U.S. can as well.
Our Conclusions about the Discussion
The paper in question has related several juicy tidbits but wholly fails to address root causes nor identify any solutions. The best we can tell is that the only people that completely cause the problem, the big, old, inefficient legacy insurance companies that waste half your premium are also the only people with all the information necessary to solve the problem.
General Conclusions
This paper so studiously ignores the entire financial elephant in the room that is health insurance, that we must conclude that The Commonwealth Fund is in their employ. Maybe we here at Sentia are the only smart people who can look at the situation and deduce that the for-profit insurance companies with their skyscrapers in every major city in the country and tens of thousands of employees and big corporate salaries and huge power consumption and networks and armies of lawyers and billions in lobbyists are the root cause of this problem, but we don’t think so. We think this is a fluff piece meant to make the unwashed masses angry at anything but the root cause: the ineptitude and greed of the bankers running your health insurance company.
The General Solution
Let’s first define the real problem. We looked at the things that an insurer needs and the things it uses to produce its service. Our analysis concluded that the insurer needs a doctor with a National Provider Number (NPI), a procedure to pay for, and a way to transfer funds to the doctor for services provided. That is it. All the big buildings and impedimenta detailed above is only used to deny you contractually obligated coverage. Your insurer keeps 47% of your premiums, on average, and returns 53% of your premiums back to you as benefits. That is almost half of your premium wasted all by itself.
If this insurer provided the Electronic Medical Records System (EMR) to the practice, you could pick up the procedures performed and pay for them in real time. Then you wouldn’t need humans at all. The coding and billing staff could be reduced to one Accounts Receivable person that makes sure that all the procedures get paid for. With this new piece of software, the insurer becomes a gently humming box in a cold room in a data center. No tens of thousands of employees, no big buildings and none of the associated costs. This solves our first assertion: Money is one of two problems with the current system
If This new software included integrated health and wellness like we discussed above, that details what is wrong with the patient, and how to correct it, plus the mental health surveys and associated worksheets and the insurer can give this package teeth by offering discounts for compliance, then We have a way to teach proper health behavior, test for proper health behavior using science, and incentivize healthy behavior by offering discounts for compliance, then we have solved our second: Education is the other root cause of the current problem.
If this new insurer wanted to make the new software a real enterprise insurance-as-a-platform solution it could add
- Secure email to confer with each other and the patient
- Self-scheduling, further reducing the need for staff at the practice/hospital level.
- Questionnaires to be fully configurable by the practice and used inside the EMR for things that aren’t structured like anything that isn’t a diagnosis, modifier, procedure or measurement. This could fully supplant the need for a specialty EMR. It could also be used for patient registration and satisfaction surveys, or anything that currently requires a clipboard.
- Reporting would be anything from an inventory report to a full profit and loss statements. This also can be used for efficacy and compliance reporting. Instead of fingering through reams of paper and making tally marks in a legal pad, you click the button and you get a report.
- Telemedicine with integrated x-ray (DICOM) viewer. Sure, you can jump on a zoom call with a colleague of a patient, but how secure is that really? Do you know? We don’t. Also, you can’t share images like x-rays or MRIs with Zoom, or any other, and you certainly can’t highlight a spot with a reticle or draw on a DICOM to highlight a particular structure.
- A fully fledged Hospital/Practice management system. You may have noticed that we referenced P&L and inventory reports earlier. These are all a part of the Enterprise Resource Planning (ERP) package that we are building to further streamline and automate healthcare delivery. This will include fully functioning human resources, accounting, inventory, capital assets and everything else that is needed to run the enterprise. Any enterprise, not just a hospital.
Cutting out billing, coding and collections, eliminating the need for efficacy and compliance reporting and providing a fully functional EMR to the practice or hospital saves the average practitioner over $70,000 per year. That will certainly push us over the 50% saving threshold.
In this article we have identified real, quantifiable problems with the US healthcare system, boiled those things down into their root causes, and given a reasonable, simple way to mitigate those root causes. Saving the consumer 50% on his or her health insurance makes us one of the most affordable globally.
We have proven also that if you show the patient what needs to be done and pay for it, they will do it, as the Influenza vaccination rates, screenings for breast and colorectal cancer, and MRI usage shows above.
Incentivizing healthy lifestyles and mental health will put us on par with the outcomes of the best in the world. Nobody else on the planet offers financial incentives to promote health. This should actually put us ahead of the curve in that regard, with a large percentage adopting the program. With Incentivizing a healthy lifestyle, the overall cost of health coverage should decrease for entire populations, further reducing the bill for health coverage.
Once we have completed the move to this clearly superior system, we will have achieved through financial incentives, a single payer system. Nobody in the country, and probably the world, will want to go back to the old spreadsheet/banker driven health coverage systems, particularly when they are double the cost. Yes, health insurance in these developed countries work exactly the same way ours in the US does, they just remove the profit motivation and run it as a government agency. That won’t work here. By removing the spreadsheets and bankers, and going to a flat rate data management system, we can start to move toward a pay-for-health or value-based system and away from a pay-for-procedure system.
General Conclusions
We have shown a way to Cut the cost of health coverage by half or more mitigating one of the root causes of healthcare failure in the US. We have shown a way to incentivize healthy behaviors and choices, mitigating the other of the root causes of healthcare failure in the US. With these two things we will be not only the cheapest medicine in the world, but also the best. We already have the best doctors and the best equipment; we just need to implement the above detailed framework to give them all the tools necessary for success.
We have this system in prototype now, fully functioning. The ERP system and the Mental Health Module are slated to start production early in 2025, but are fully designed and the databases built.
Contact us here or on our site and we will be happy to provide a demonstration of the fully functional prototype.
If you liked what you read, please like and subscribe, click on the notification icon, subscribe to our newsletter, and follow us on all our social media and blog sites.
We have built a comprehensive health information system to keep the patient healthy and on the right track with the ability to incentivize healthy living. Implementing this system should be fairly simple and will completely revolutionize the way healthcare is paid for, saving countless lives. We have shown a way to use this system to make the best healthcare system in the world also the most efficacious and the most affordable, and a way to move toward value-based care.
Comment
| Date Written | Comment |
|---|