How to Build a Universal EMR
A deep dive into functionality (Part 1)
Introduction
Over the past few months, we at Sentia have been advocating to streamline and automate health insurance. We have stated that this is accomplished through providing the Electronic Medical Records System (EMR) to the practice or hospital. That is only viable if we can provide an EMR that is at least as good as what is available now. We think we can do that better and we are going to present our case today. In subsequent installments in this series, we will explore the technology, the security and interoperability, but today we will focus on what this system does, not how. Since all our processes are automated, we can charge $10 per month to the patient plus the actual cost of the risk, eliminating about 50% of the cost of traditional insurance, plus another 25% for lowering the incidence of chronic disease.
Functionality
The base functionality of the EMR is broken down into eight categories:
- The EMR itself.
- Integrated health and wellness – We provide patients with a portal that scientifically analyzes the annual (semiannual, quarterly) checkup and prescribes patient education on how to live healthier, better, and longer.
- Integrated Email – We give the patient the ability to contact the doctor via SECURE email.
- Self-scheduling – log in and see when your favorite practitioner is available and schedule a time to meet.
- Questionnaires – Practices have the ability to design, assign and read questionnaires online. This means you as the patient don’t sit in the waiting room with sick people filling out reams of paperwork. Additionally, this system is part of the EMR itself to customize the system for each practice, according to their own specifications.
- Reporting – Individual and Population Health Analysis: the individual gets a printable report of his or her health as it was recorded on the date of the health assessment. Population Health reporting gives the practice the ability to see how they are doing. Efficacy and compliance reporting becomes a one click report instead of a weeks long stare and compare in a spreadsheet. Estimates of patient responsibility.
- Compliance – as this product matures, we will be able to differentiate between people who live a healthier lifestyle and those do not by comparing the individual’s metrics against themselves over time. Those who make demonstrably better decisions will pay lower premiums than those who do not, based on personal metrics.
- DICOM Viewer/Growth Charts – attach images and documents to the medical record, and generate and save growth charts dynamically based on measured values.
The Record Itself
Our EMR is based around the patient. The first order of business is to select a patient.

This is fairly self explanatory but also of note that we use a multitenant database. This means that there is one record for every patient, no more and no less, so you can search for and find patients that have never been to your practice before.
Next we can select patients that match the criteria we typed in the previous step.

Our test subject, John Q. Public is selected. We select “Encouters” to see his records.

Things to note here: there is a list of Jack’s Health Risk Assessments at the top for reference. The list of actual visits is below. Selecting one of them will return this:

Apologies for the small size, there is a lot of information here. First is a detail of the measurements detailing health such as height, weight and blood pressure. Aberrations from normal are highlighted according to their abnormality in yellow or red.
Next we have four sections that comprise a SOAP note (Subjective, Objective, Assessment and Plan) section to document the patient encounter. These are not typed, they are picked for ease of entry and accuracy. It is actually faster to search and pick than to type and far more accurate.
Under that is the note itself. This is populated from the choices you made in the four sections above it and again, no typing is required.
Let’s click the add button in the first section and see what happens.

This is the UMLS selection tool. You can search the SNOMED_CT (discussions about this are for a subsequent article in this series) according to concept type. As you type a write ahead drop down will populate.
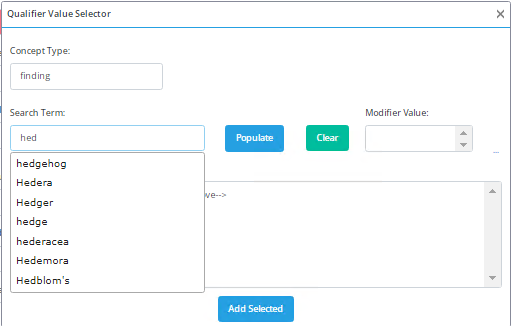
Notice here that the search term was not found so we will click populate to find out how to spell what we were looking for.
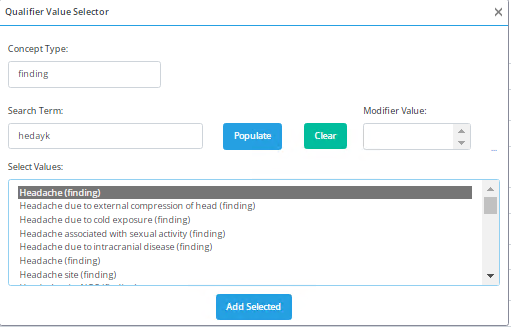
Notice that the spelling was corrected and the thing we wanted is at the top of our list.
We can also modify this finding by clicking on the ellipses to the right of the Modified value list box

This allows the practitioner to modify the selected value and then add it to the SOAP Note. the resulting generated soap note looks like this:

These are all discrete values picked out of a database so they are 100% searchable and we can create aggregate reports and queries that search for these values or combinations of values. That means that we can pick a differential diagnosis and get a list of associated symptoms that others have found in the past, or give a list of symptoms and get diagnoses that match. This makes Dr. House look pretty silly tottering around on his cane and thinking hard enough to make smoke come out his ears.
Next, the practitioner CAN type in free form notes to remind themselves and others of relevant information outside the main soap note.

For the main medical record, that is really it.
Again this is based on the UMLS that is updated twice per year and ingested into our database. It is suitable for any medical eventuality, and in fact, unlike ICD and CPT codes, was designed to document patient encounters in their entirety.
Additionally, not pictured, we have a Survey tool that we will integrate with the EMR that will allow a practice to build a questionnaire to request additional information that is attached to the record. These are not UMLS values, just questions the practice wants to ask at a given time in the process, allowing them to ‘modify’ the EMR to suit their own needs. The practice writes the questions and the system saves the answers. More on this in the Questionnaire section of this document. One of our Ambulatory Surgical Centers (ASCs) uses this survey to record blood pressure, heart rate, etc., when the patient is handed off from surgery to recovery.
Integrated Health and Wellness
84% of all spending on healthcare in the US is made on avoidable, behavior based chronic disease. That means that in 2024, of the $4.7 trillion we paid for healthcare, $3.95 trillion was spent on available disease. Americans are about ⅓ more likely that other developed countries (OECD) to have avoidable disease. The OECD average mortality due to chronic avoidable disease is 225, the US averages 336 per 100,000. If we get Americans healthy, at least to the point where everyone else is, we could save $1.27 trillion. At Sentia, we have developed a system that
- Tells you what is wrong with you
- Shows you how you compare with acceptable values
- What to do to correct the problem
If the patient logs in and even looks at the prescribed patient education, he or she gets a small discount. If they see how to correct identified problems, they get a large discount.
Let’s look at our test patient’s Health Risk Assessment, the Individual Health Analysis and the prescribed Patient Education
Health Risk Assessment Page 1:
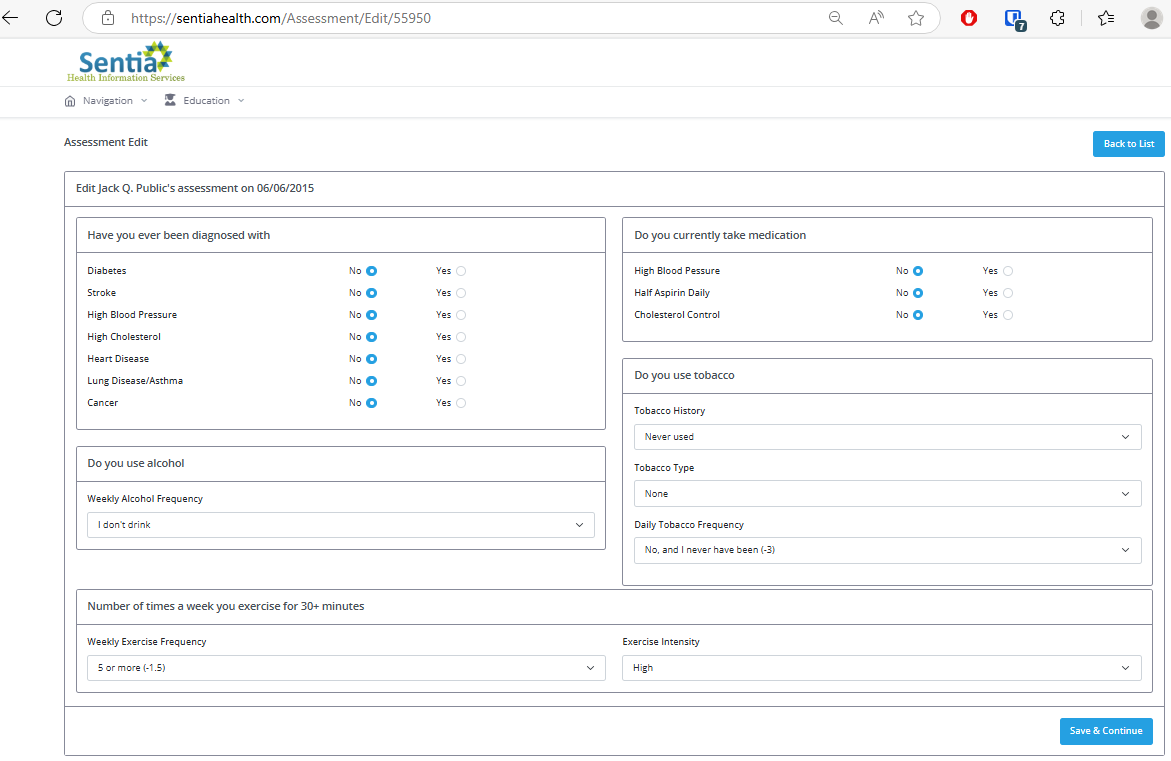
These are the history and behavioral questions we need to construct a health risk assessment, also included is a mental health assessment on page two:
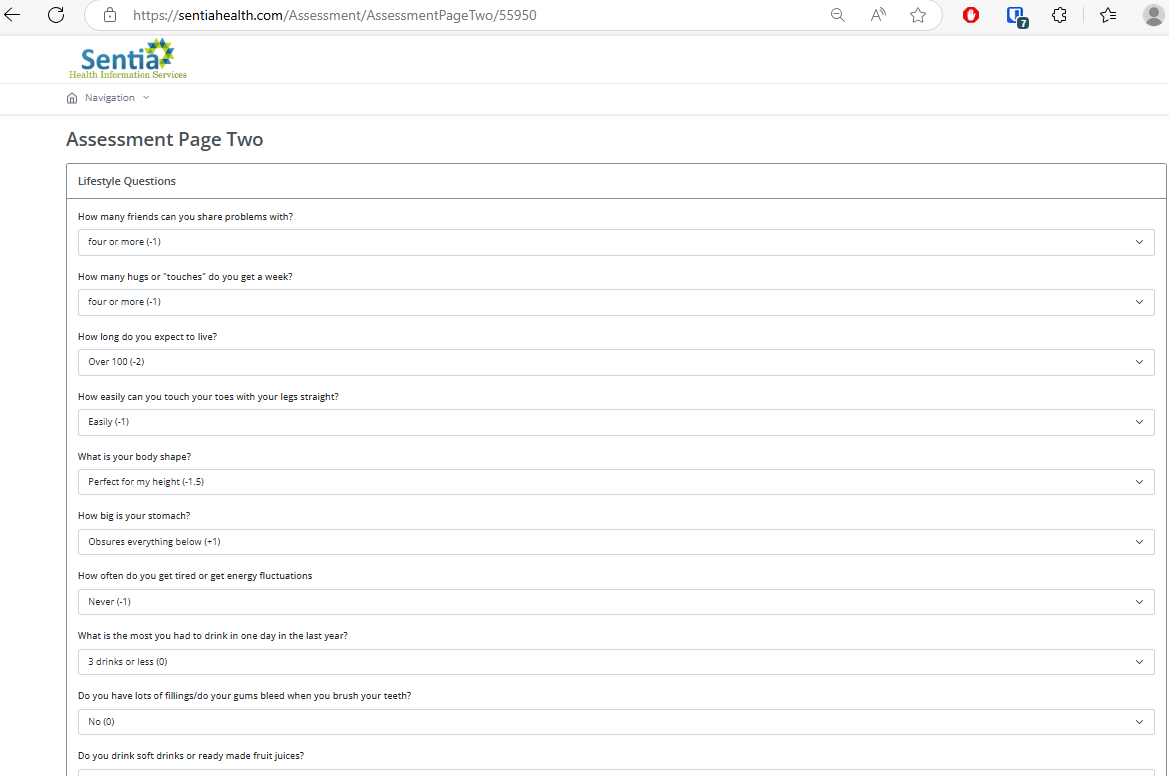
Finally, the regular checkup, a regular patient encounter, filled out by clinical staff. Note the previous sections are filled out by the patient, anywhere in the world that has an internet connection.

Now all we need to do is report back to the patient, as we discussed, so they will know what is wrong and what to do about it.
Here is the printable Individual Health Risk Assessment
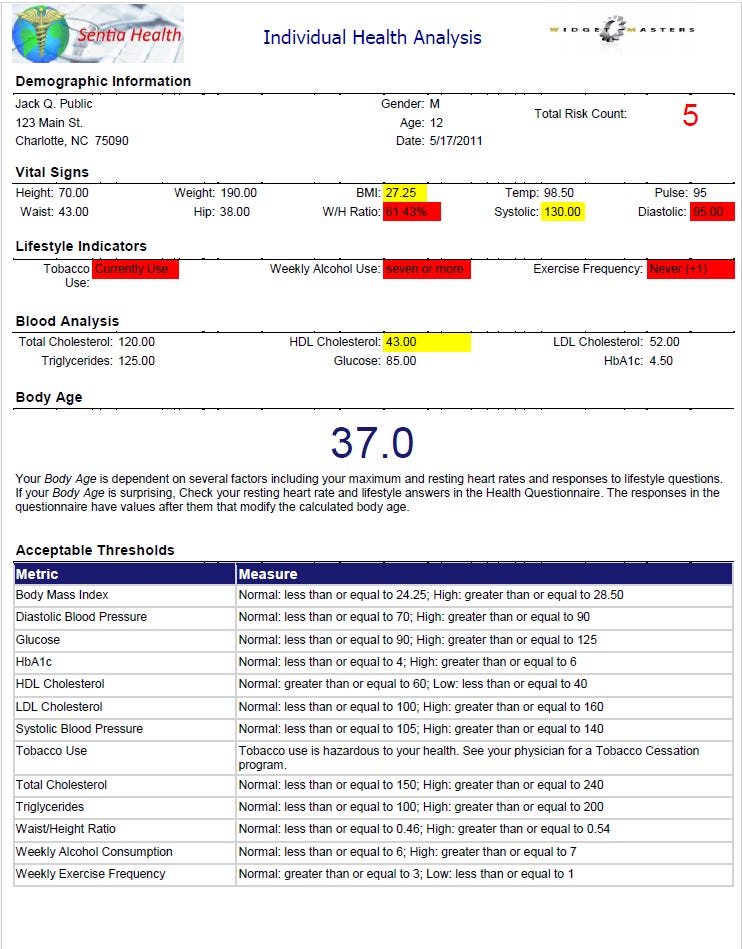
There are several things to note here. First is our total risk count. This is the number of results that are out of normal range that the patient needs to focus on. This is a printable report available online as well, that gives the patient an overall view of what needs to be done. Second, note the actual age of the patient and the Body Age. this is derived from the Uth, Sorensen, Overgaard, Pedersen equation and is intended to scare the patient into moving around a little bit.
Below is a copy of some of our patient education that is automatically prescribed when the lab results come in.

Things to notice: the temperature gauge shows how far out of normal your results are. The range for normal readings. A problem statement and a solution statement that details what to do about your condition. Finally, a link to further education on a free site (in this case WebMD.com) for more information. We have contracted with Krames to provide patient education materials for the patient in the case of things we don’t have written documentation for ourselves. This is our plan to save the $1.27 trillion we talked about earlier. We quite literally bribe the patient to get up and move around with things like the body age, the temperature gauge and some cash to lower the cost of their individual insurance.
Integrated Email
You can’t send sensitive medical information over email. Because of that, we have developed an integrated ‘email’ system to transfer this information in a more secure manner.
It works exactly like you’d think and is fairly easy to show.

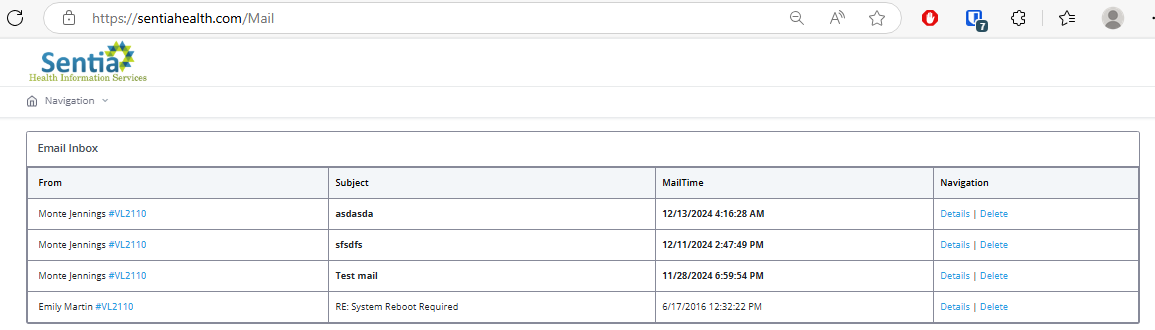
This should be fairly intuitive to use and works as you’d expect.
Self Scheduling
Scheduling is available to the practitioner, the staff and the patient to make a new appointment from the patient encounters page, in a menu at the top. It looks like this:

Clicking the “view times” button results in the details page where any of the above people can schedule an appointment:
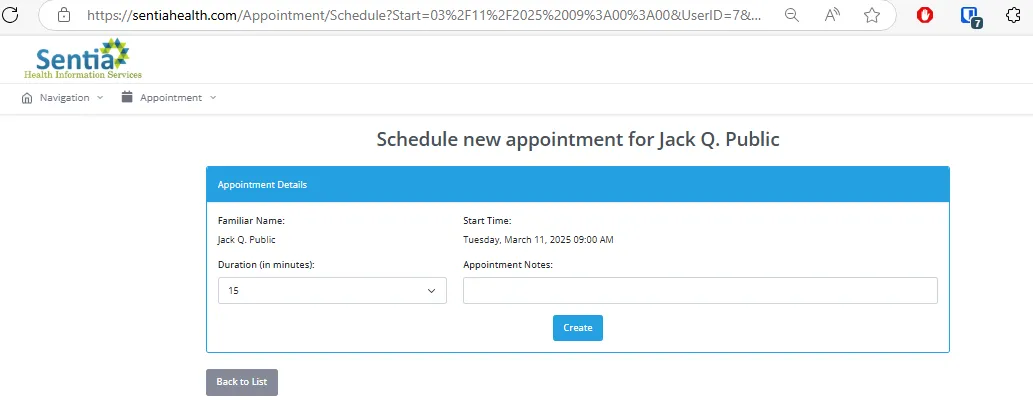
This is based on the practitioner’s schedule, so we don’t have appointments when that person isn’t at the clinic/hospital. Showing the scheduling administration is beyond the scope of this presentation, but it is there and it works.
Questionnaires
Normally, when you visit the doctor, you have to sit in the waiting room with a ream of PAPER and a PEN filling out the same information over and over. Name, address, phone, date of birth, and then have to actually fill out the forms that have been run through the copier ten thousand times and are barely legible. Now all that is gone. We provide the practice or hospital a way to design and build their own questionnaires with no programming and no additional assistance at all. Type the question, select the answer type, and click publish, and your survey is live on the internet, ready to be assigned to a patient or to an encounter. Further, the questionnaire is viewable as a printable report, suitable to give to the patient or save in a (shudder) file cabinet. Below is a test questionnaire commissioned by an MRI practice:

Think of the Questionnaire tool like a medical SurveyMonkey, a $3 Billion company, except that this is HIPAA compliant, secure, and no additional cost, outside of the $10 per month paid by the patient.
Reporting
We’ve mentioned the reporting tool several times. Let’s dig into some details of what it is and how it works. Currently, the reports are only available to design by the development team. We have several available and you have already seen a few examples. The value this brings is mostly formatting. We run the data extraction for the report and pass it in as a data table that is consumed and displayed by the report itself. The report is then savable as Excel, Word, PDF or any of a number of other formats, or simply printed out. Here is an example of our fully automated Population Health Report (page 3), just click the button and open the report.

Notice the built in table of limits and the bar chart showing the number in each category of this particular population. This is a 27 page report generated in a few seconds, and a test copy is available on request.
Compliance
Compliance, in this case, measures what the patient is doing to maintain his or her health. While this is on an individual level, and thus can’t be shown here, and is only used in other calculations, like discounts for healthy living, we do have a population compliance report that details how individuals are tracking in health over time and against only themselves. This is a copy of the first page of a compliance report pulled for one of our clients (and one of their clients) not too long ago:

There are of course several pages to this report but for brevity we only captured the first page.
Built In DICOM Image Viewer/Growth Charts
Inherent in every record is an image and growth chart viewer. This is separate from the DICOM viewer below that is for sharing images, though the patient and anyone with access to the records can view these.


Conclusion
In previous articles we have shown a way to save 50% now and an additional 25% eventually of the cost of health insurance using our own EMR. This is that EMR. This is the sine qua non for our new plan. We welcome your feedback in our efforts at continuous improvement.
We have shown a way to make patients healthier by educating them on the consequences of their behavior, and a way to capitalize on that to the sum of $1.2 trillion or about 25%. If we add that to the process automation savings of our solution, we are in the ballpark of more than 75% savings in total. We already have the best doctors and the best equipment; we just need to implement the above detailed framework to give them all the tools necessary for success.
We have this system in prototype now, fully functioning.
Contact us here or on our site and we will be happy to provide a demonstration of the fully functional prototype.
If you liked what you read, please like and subscribe, click on the notification icon, subscribe to our newsletter, and follow us on all our social media and blog sites.
We have built a comprehensive health information system to keep the patient healthy and on the right track with the ability to incentivize healthy living. Implementing this system should be fairly simple and will completely revolutionize the way healthcare is paid for, saving countless lives. We have shown a way to use this system to make the best healthcare system in the world also the most efficacious and the most affordable.
Comment
| Date Written | Comment |
|---|